Cabotegravir and Rilpivirine long acting injections were launched in UK ( a few days back ) for treatment of HIV. The same was earlier approved by USFDA in Feb 21.
The current cost of this treatment ( this injection is administered once every two months ) is very high… estimated at Rs 1.4 lakh / month vs the traditional ARV combo - TLD tablets that cost aprox Rs 700 per month.
I understand that the new treatment can’t go a long way in LMIC countries at present prices.
However… Is this not a long term threat for Laurus’s ARV API and formulations business ???
What happens when this treatment goes off patent ??? Won’t the mkt de-value Laurus’s ARV business as its terminal value would seriously erode because of this development ???
Or is it that I am missing something here ???
I request senior Valuepickrs to please throw some light here.
A cost-effectiveness analysis has found that injectable, long-lasting antiretroviral therapy (ART) would need to cost no more than $131 a year in order to be cost-effective if used for patients who are not fully virally suppressed in lower-income settings in regions like sub-Saharan Africa.
The analysis found that injectable cabotegravir/rilpivirine would only reach the threshold of cost-effectiveness, defined as $404 per disability-adjusted life year averted, in people who had viral loads over 1000 on standard oral ART. The price of oral ART was considered to be $78
At present, the injectable therapies are very expensive. A US list price of over $48,000 a year was quoted by the New York Times the day Cabenuva was licensed, while a recent cost-effectiveness analysis of injectable PrEP used Cabuneva’s Canadian list price of $25,800 . These prices are likely to fall as discounts are negotiated.
When used as ART, studies found that injectable cabotegravir/rilpivirine was as effective as comparison oral therapies but not more so.
I think in terms of affordability in the west , that is not much of a concern.
In UK, NHS is free , state take care of healthcare, in USA it is more of insurance based so more or less the cost is not a problem. And I am sure it is more or less same in Europe as well.
For sure there is still lot of demand in LMIC countries.
I think we have to look this in a different way, experts like @hitesh2710 can shed some light on this and enlightens us with their knowledge.
If X person is infected with HIV
What is the total duration of the treatment? (is it life time ? )
How much it costs every year ? Current dosage form vs Injectables
ImmunoAct
The bigger picture we have to understand from the recent acquisition is they are entering into cell based treatments eco system.
This is my understanding (Bigger Picture) and open to learn from other boarders
I am trying to connect the dots
Health Care Global has the Data (They are the cancer specialists , they are building the database of various cancer mutations to offer precision treatments )
We have these companies (like ImmunoAct , Syngene that are bulding technology platforms for innovators ) that are working on cell based therapies once they have a solution that needs to be validated against these various mutations
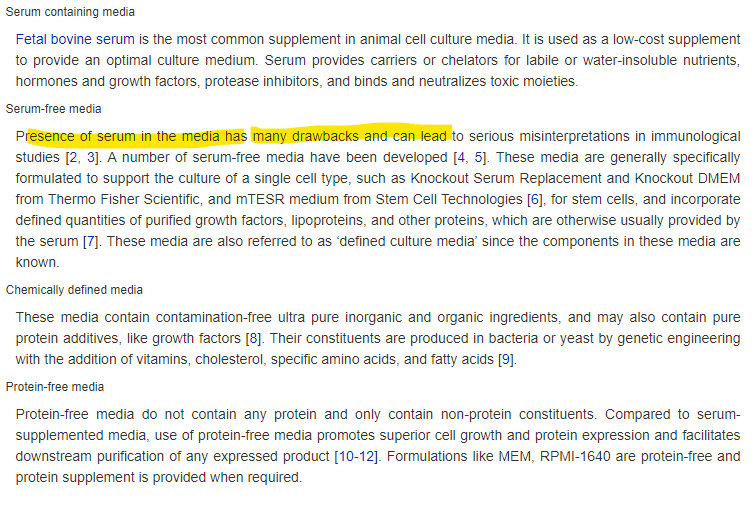
To work on cell based cultures we need media to grow the cells , Mr Chava did mention this many times (Thermo Fisher is the leader in these and there is huge push for non bovine serum based media ) , we need to understand Richcore (Laurus Bio ) is producing any such products ? This will be a backward integration kind of things for ImmunoAct ?
In 2018, the preferred first-line treatment of the fixed dose combination (FDC) TLD was available at $75 per patient per year.
In 2016, AZT/3TC and ATV/r were the cheapest generic second-line drugs at a cost of $286 per patient per year,
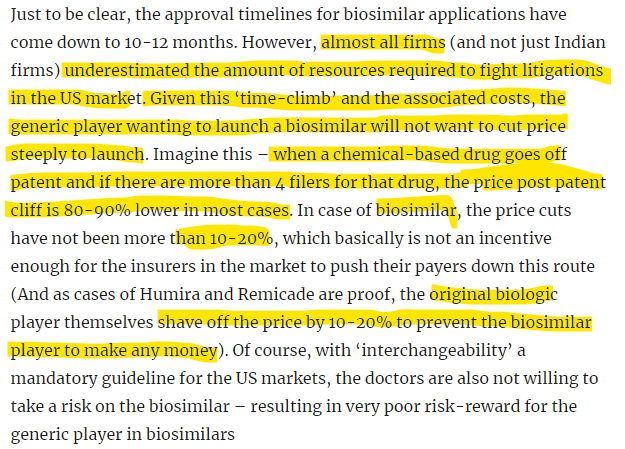
The below snippet is from ace investor Kiran, for me this is an eye opener how to look at various pharma companies especially the ones that has more exposure to regulated markets.
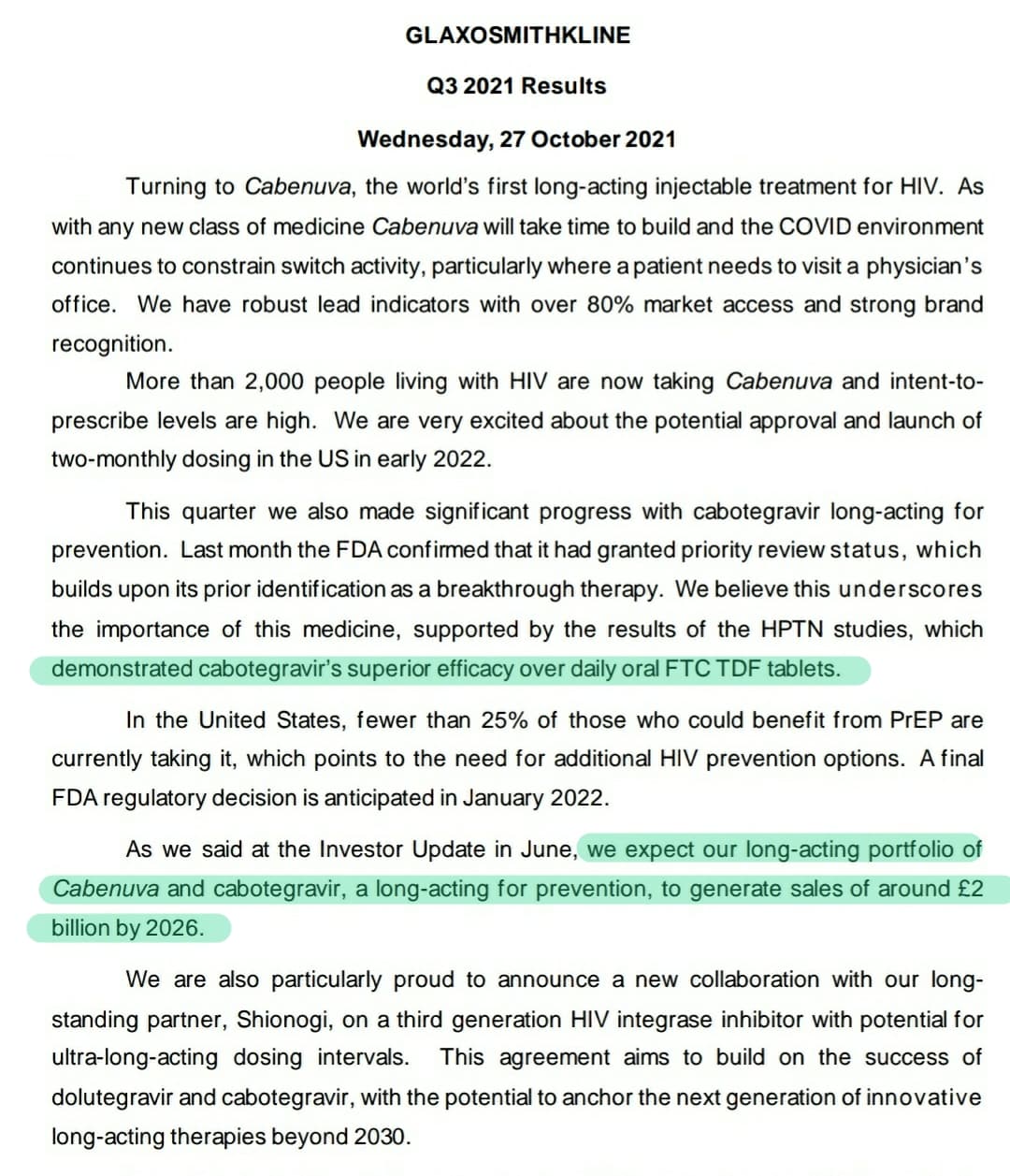
Recent study published on New England Journal of Medicine has found that Cabotegravir injection(2 monthly) is superior to current ART regimen in pre exposure prophylaxis of HIV in high risk individuals.
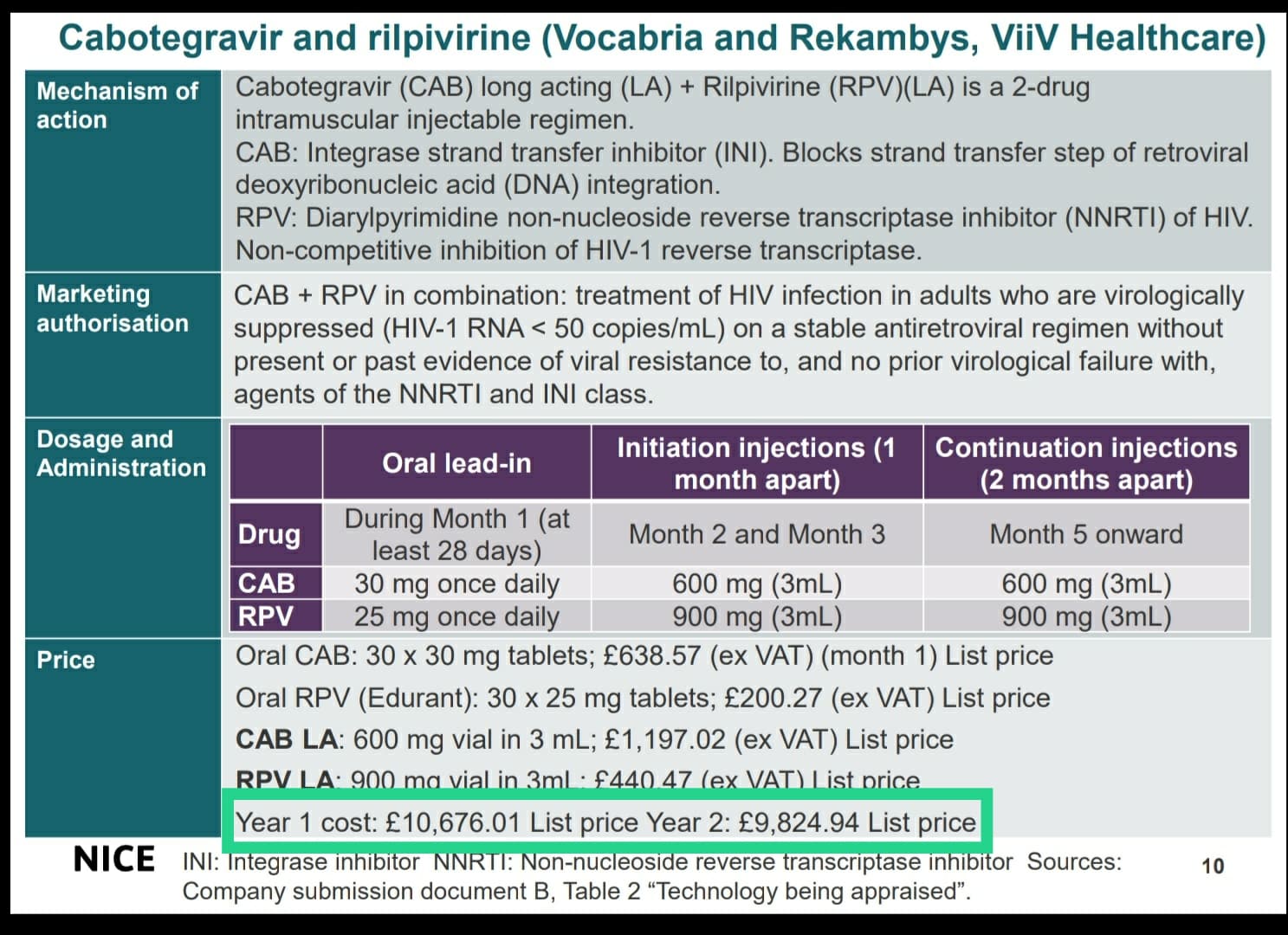
List price of Cabotegravir + Rilpivirine for an year costs €9824 ($11068). Bulk orders by the government ‘may’ acquire drugs below the list price. Since it is a 2 monthly injection, only 6 doses are needed annually.
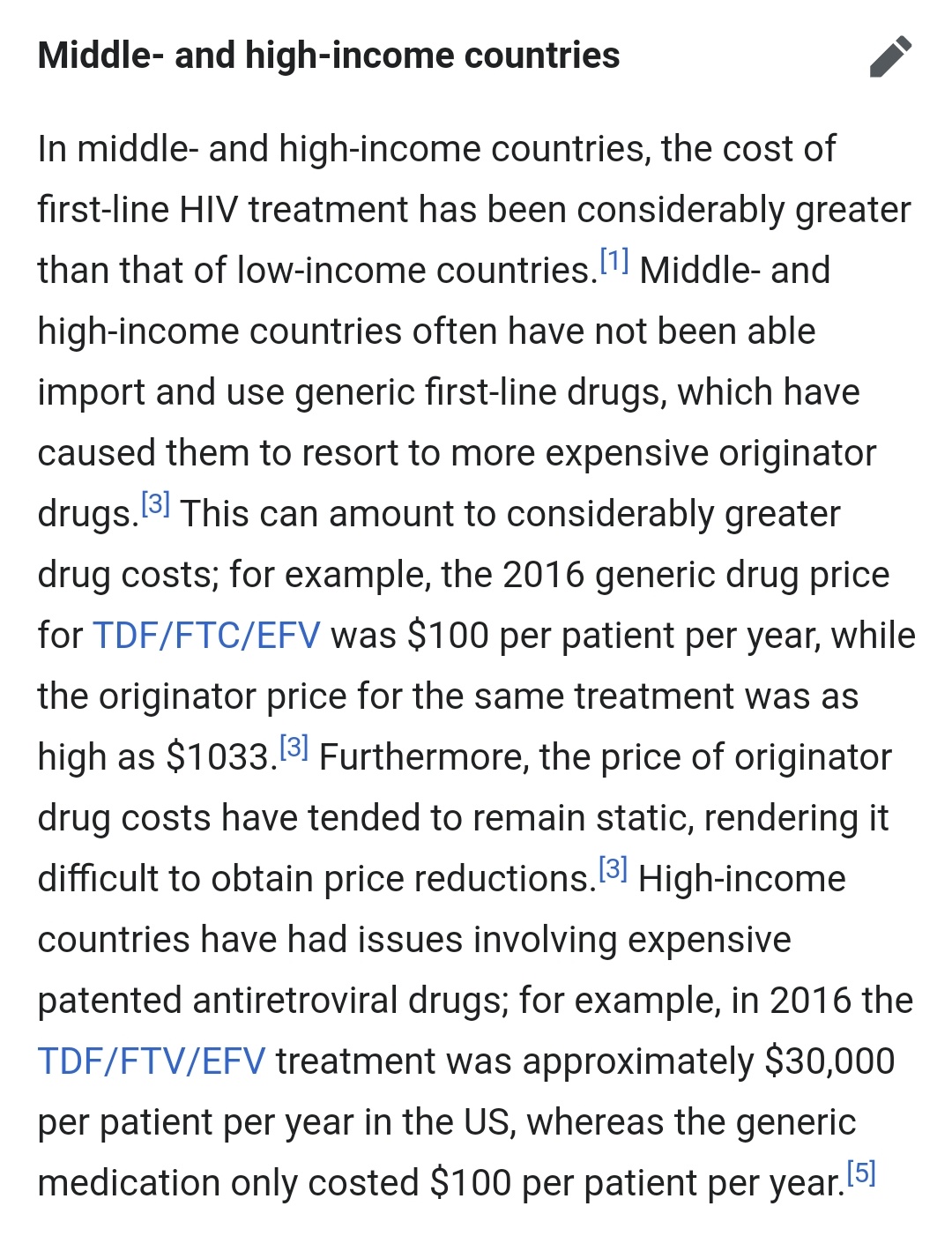
Current treatment regimen in US costs $42,000 annually. Comparing to this, Cabotegravir+Rilpivirine is a cheaper.
This high price is because middle & high income countries are not included in voluntary licensing agreements and they must pay high prices to orginator companies for patented drugs.
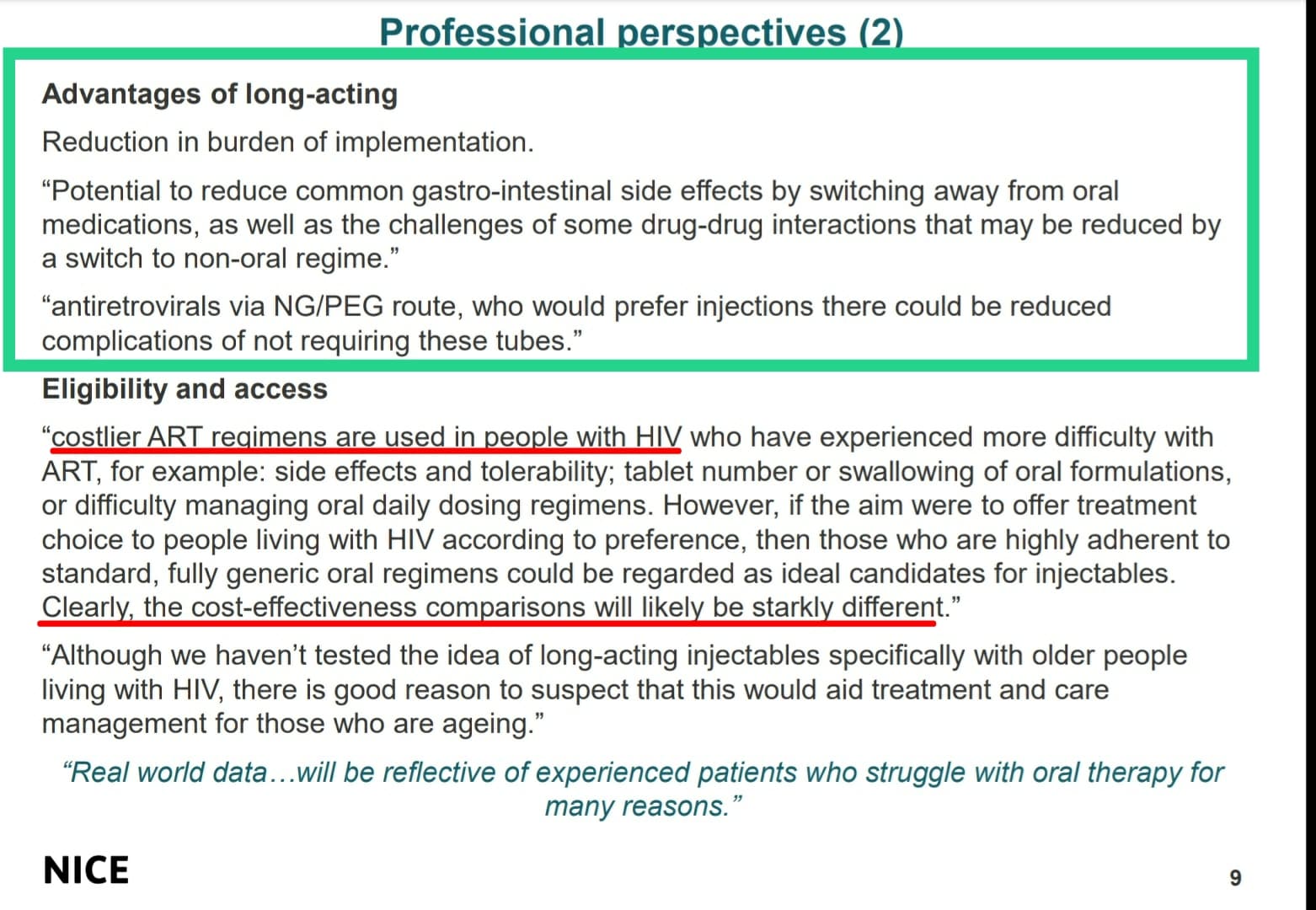
Comparing to the current treatment regimen of daily oral intake throughout the lifetime, Cabotegravir+Rilpivirine is only needed to be taken 6 times a year, which provides greater comfort to the patient and reduces social stigma associated with taking ARTs daily. This helps the patient to adhere to the treatment and reduces suboptimal adherance to ARTs. Unlike current oral therapy injectables also has no gastrointestinal side effects. These factors may compel the ART clinics to shift to newer regimen apart from cheapiness in cost in US.
Injectable Cabenuva has high potential on Pre exposure prophylaxis(PrEP) of HIV infection in high risk individuals (health care workers in HIV management, sex workers,etc). Latest study shown it’s superior efficacy over current oral therapy. Also patients only need to take injection once in every 2 months as PrEP unlike current daily regimen. In US only less than 25% of target population (already mentioned high risk individuals) is currently taking PrEP. With this bimonthly prophylaxis option, more people will opt for it. Viiv expects to make € 2 billion by 2026.
Thanks for sharing this info. Any idea why does the price cuts of biosimilar are limited to 10-20% only then the original biologic? Wouldn’t the material cost and other overheads leave more room for the biosimilar players specially from countries like India to have them priced at almost half the original biologics and still make some decent margins ?
The answer is not straight forward (Read Mr. Kiran summary again why after the patent expiry copy cat biosimilars are not entering into the market ? )
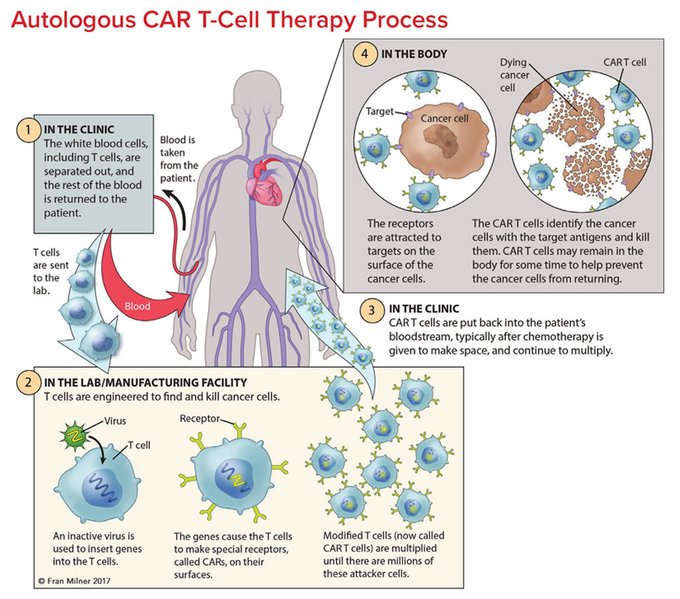
Cell based therapies are not one solution fits all , it has to be tailored (based on the patient own cells) and then inject into patients body.
People who has deep understanding of the entire value chain of these kind of treatments can answer this question. Based on my little knowledge this is what I understood so far.
Assumption : Treatment is readily available (for example Car T cell therapy for blood cancer , by innovator based in US or India )
If the treatment is costing $150,000 in US the same cannot be reduced to $20,000 even if the innovator does the tech transfer to an affiliate in India, why ?
The equipment, the lab, human resources , consumables used to grow the cells are expensive, the only cost advantage if at all we can achieve is labor cost other than that rest of the things are mostly imported ( equipment , cell culture media )
There are many steps the treatment has to go through to the final stage where the engineered cells are injected into patient, in any of those steps if the QC fails (cells are contaminated or not seeing the desired results ) then the entire process has to be started again.
Automation, advancement in technology can bring down cost , even competition where companies from india( recently initiated National Biopharma Mission) can play significant part
A new therapy called Off-the-Shelf CAR-T is promising cost wise as well , but Still Years Away from the Clinic.
Cabotegravir long acting injectables are an approved treatment for PrEP. However, most of the HIV patients are PEP where Cabotegravir has not been approved and at present Oral ARVs are the only option.
Is this understanding correct or is there something that I may be missing ???
Thanks for sharing this info. Can u also share the source of this info…IE cabotegravir being approved for PEP also
Also…if you can throw some light on …Is Cabotegravir approved for treatment of Acute or Chronic HIV infections ( Actute and Chronic stages are reached after the Pre Exposure and Post exposure stages…as per my understanding of progression of HIV infection )
I m probing as I am an interested party and want to know more about the issue
Please don’t mind
Also correct me…if I am wrong as I am not a medical professional
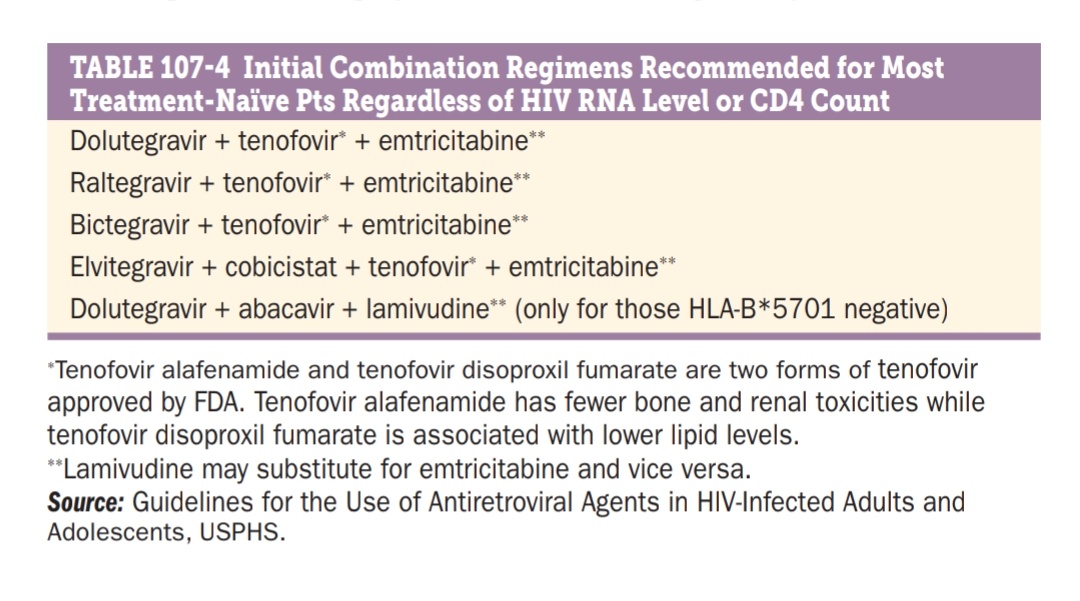
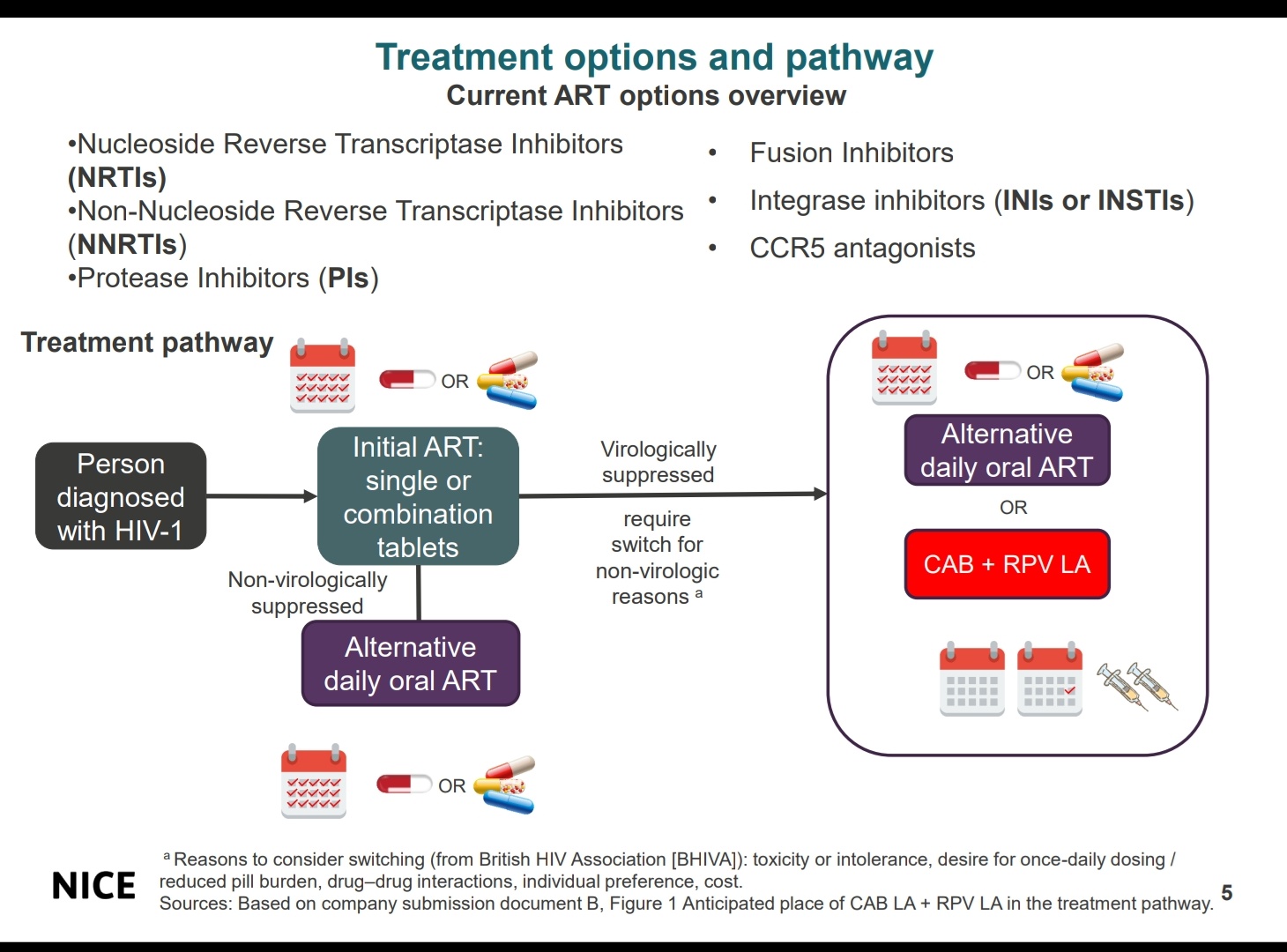
There is no such thing as different therapies for acute and chronic stages of HIV infection. Once the patient is diagnosed to have HIV, then the patient is started on combined Anti-Retriviral therapy.(Usually a combination of 3 drugs, 2NRTI +1 Integrase inhibitor).
Goal of the combinedART therapy is maximal suppression of viral replication and eventually maintain the serum HIV RNA level < 50copies/ml. If the therapy we have given is effective, CD4+ T cell count will rise.
Selected combined ART regimen is continued till resistance to any of the drugs is developed & manifested as decline in patient’s CD4+ T cell count or failure to achieve and maintain an HIV RNA level <50 copies/mL. These are indications to consider a change in therapy (Patient will be shifted to another combination of drugs). Drug regimen switch can also be considered in case of drug intolerance (adverse effects), drug interactions with other drugs, patient’s preference, cost etc
Similarly cabotegravir is also combined with another drug Rilpivirine to prevent development of drug resistance. Now NICE (National Institute of health & care excellence) has approved combination of Cabotegravir+Rilpivirine for the treatment of HIV and for pre exposure chemoprophylaxis.
Current guidelines allow the drug switch to Cabotegravir+Rilpivirine in those patients who are already virologically suppressed by initial combined ART.
The crux of HIV treatment is to suppress the serum HIV RNA levels as low as possible (<50 copies/ml) and improve the CD4+ T cell levels and treat any complications which arises.
In the presence of Minister @KTRTRS, Principal Secretary @jayesh_ranjan, Govt of Telangana today entered into a consortium agreement with @drreddys and @LaurusLabs for setting up a Centre of Excellence on Flow Chemistry.
@ShakthiNagappan, Director for Life Sciences and Pharma, G.V. Prasad, MD @drreddys, Dr. Satyanarayana Chava CEO, @LaurusLabs, Dr. Srinivas Oruganti Director, Dr. Reddy’s Institute of Life Sciences have signed the agreement respectively.
But CMO or CDMO can be expected as cost will be at least 40-50% lesser than developed nation, as fixed cost will not rise but revenue can have a hockey stick growth